















 24 / 103
24 / 103

R
uschel
LG
et
al
.
308
R
ev
A
ssoc
M
ed
B
ras
2017; 63(4):307-310
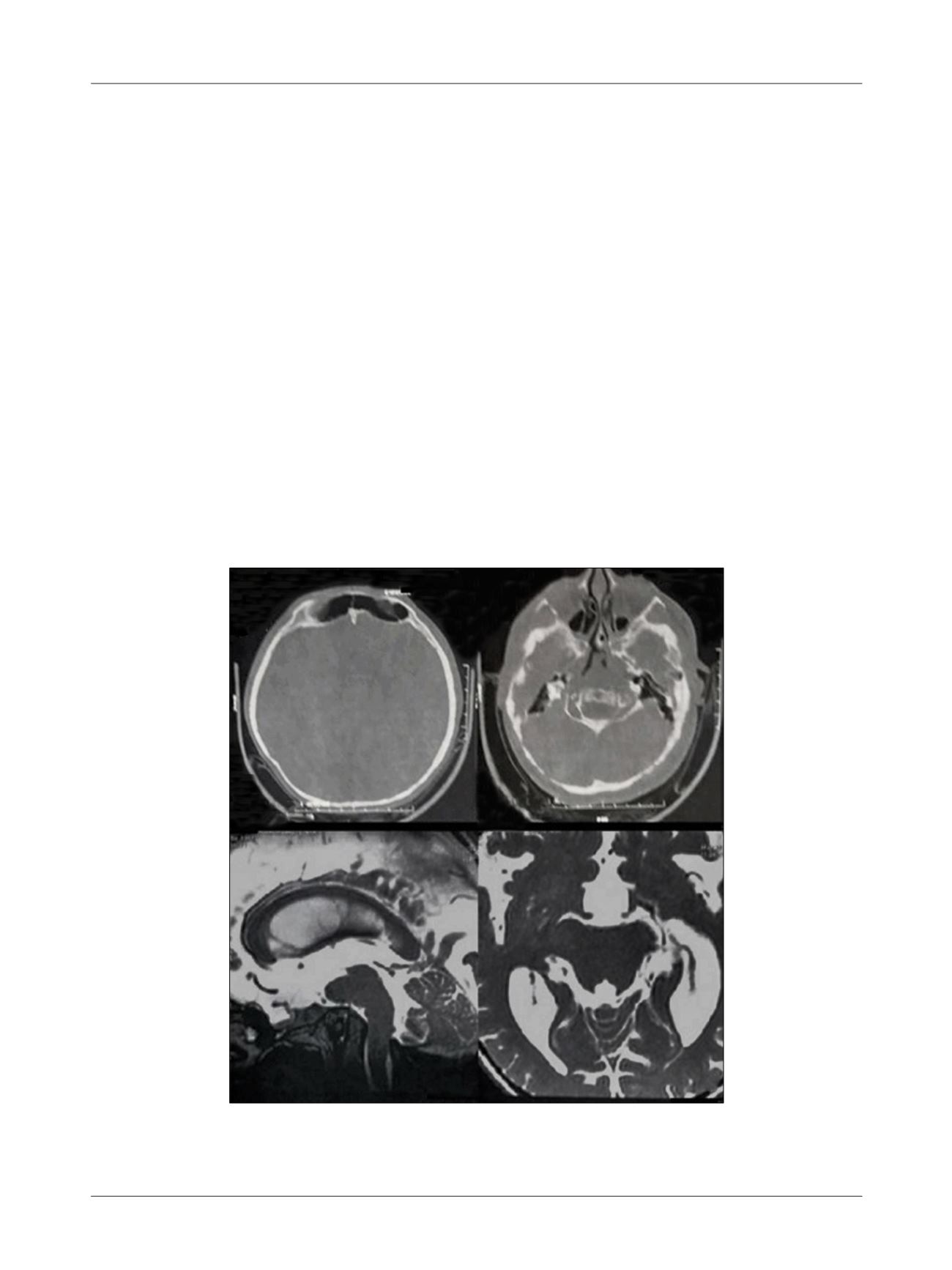
FIGURE 1
A. Wormian bones in a brachycephalic skull. B. Skull base abnormality. C. Basilar invagination obliterating the prepontine
subarachnoid space, with compression of the brainstem. D. FIESTA image depicting the cisternal portion of the left trigeminal nerve.
Magnetic resonance imaging (MRI) revealed basal
angle (Welcker) enlargement and clivus almost parallel to
the palate, denoting platybasia. Remarkable basilar in-
vagination was present, with odontoid process projecting
17 mm and 27 mm above the Chamberlain’s line and the
McGregor’s line, respectively. Significant dorsal insinua-
tion of odontoid process was found occluding pre-pontine
subarachnoid space and compressing the pontine-medul-
lary junction (Figure 1). No mass lesions or contrast en-
hancement over the fifth cranial nerves were seen.
Cranial-CT scan showed brachycephalic skull, with
thin and irregular skull cap. Both foramina ovale showed
irregular shape and reduced diameter.
The procedure was performed using angiography
suite, allowing easier visualization of the foramen ovale.
Under light sedation and with the patient in supine posi-
tion, with slight neck extension, the X-ray intensifier was
positioned on submental view to obtain the images fol-
lowed by 3D CT-scan in the angiography suite. A #15
gauge cannula was inserted and positioned at the foramen
ovale prior to a #4 Fogarty embolectomy catheter. The
X-ray intensifier was displaced to lateral view and inflation
was performed (1.0 mL of radiopaque dye). A pear-shaped
image was obtained and the patient developed transitory
bradycardia response. Position was confirmed with 3D
CT-scan (Figure 2), balloon was deflated, process was
repeated twice for 3 inflations (20 seconds/each, total 60
seconds) (Figure 3). No neuronavigation system, Mayfield
clamps, frames or stereotactic devices were used.
Post-procedure, the patient reported painless hypo-
esthesia on left V1, V2 and V3 segments. She was discharged
pain-free on the same day, with instructions to maintain
the medication dosage until her first medical appointment.
After one year of follow-up, the patient no longer com-
plained of pain and ceased taking all medication.
D
iscussion
OI can be characterized by bone fragility secondary to
reduced bone mass.
2,3
Fortunately, this clinically and ge-
netically heterogeneous group of heritable disorders is
A
B
C
D