














 91 / 96
91 / 96

S
ickle
cell
retinopathy
: A
literature
review
R
ev
A
ssoc
M
ed
B
ras
2017; 63(12):1100-1103
1101
observed at the periphery of the retina, resulting in unper-
fused and presumably ischemic areas. Retinal neovessels,
in turn, tend to develop in these areas, but not necessarily.
14
Individuals with SCD as well as sickle cell trait (AS) are at
increased risk of developing increased intraocular pressure
when they present with hyphema (bleeding in the anterior
chamber of the eye).
12
Low fetal hemoglobin (HbF) is gen-
erally associated with increased intravascular sickling and
is responsible for several vaso-occlusive complications in
homozygous SS.
15
In addition, Roy et al. associated prolif-
erative retinopathy with low levels of HbF.
16
Another possible change cited by Ballas et al.
11
is glau-
coma, due to high ocular pressure caused by clogging of
the trabecular meshwork and the inflow of aqueous humor.
Vaso-occlusion leads to optic nerve damage, causing visual
impairment even before the occurrence of retinal changes.
17
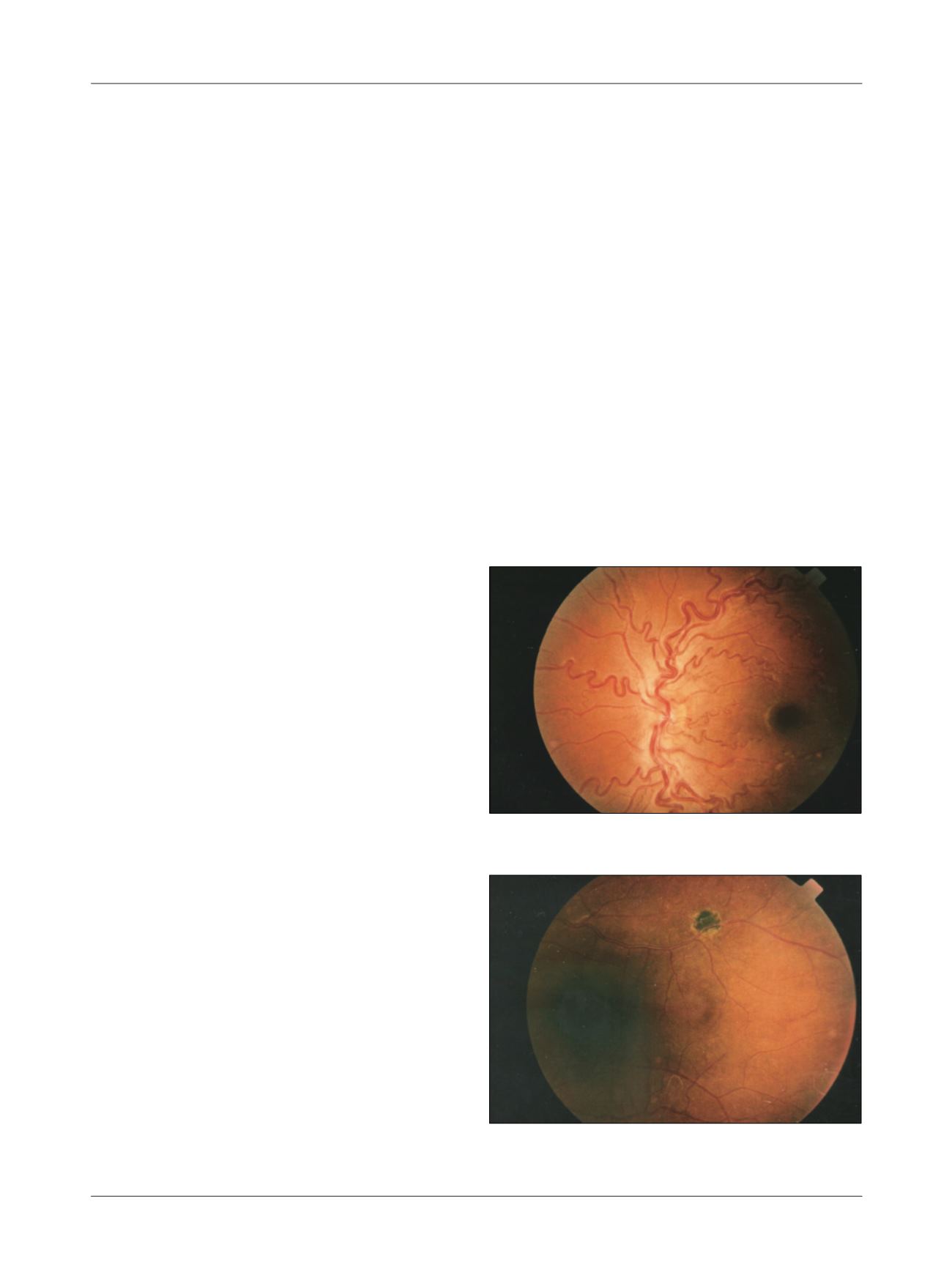
Non-proliferative retinopathy can occur with small
intra-retinal hemorrhages, possibly due to ischemic vessel
wall necrosis, called salmon patches; the bleeding then
becomes yellow and then white, disappearing without a
trace. There may also be hyperpigmented lesions in deep-
er or sub-retinal hemorrhages, called black sunbursts
(Figure 2).
12
Maculopathy occurs as a result of chronic
changes in the perifoveal capillary network.
8
According to David et al.,
1
there was macular change
in 14.4% of the patients. However, Clarkson found 4.6%
of this same type of lesion. Both found higher prevalence
in the SS type.
Although proliferative retinopathy has the same
genesis as nonproliferative retinopathy, their progression
differs. It was divided by Goldberg in five stages,
12,18
cor-
relating them with their order of appearance: Stage I is
characterized by definitive arteriolar occlusion, with
consequent retinal hypoxia and rearrangement of adja-
cent capillaries. In the next stage (stage II), the budding
of new vessels begins, with possible dilatation, aiming
to join the vascular and avascular retina. In stage III,
under the action of angiogenic events, pre-retinal neo-
vascularization occurs, forming the so-called retinal sea
fans.
12
These new vessels develop from arteriovenous
loops or crossings, and often undergo self-infarctions
probably caused by the unusual characteristics of the
flow. The new vessels are fragile, immature and adherent
to the vitreous. This facilitates the occurrence of vitreous
hemorrhage and characterizes stage IV of proliferative
retinopathy in sickle cell disease. When bleeding reach-
es the visual axis, it causes scotomas and amaurosis. The
repetition of these hemorrhagic phenomena leads to
rupture, retinal detachment and vision loss (stage V), the
final stage of sickle cell proliferative retinopathy.
12
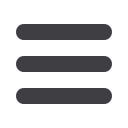
Sickle cell retinopathy develops in up to 42% of sick-
le cell individuals in the second decade of life.
10
Vascular
tortuosity is the most common finding (Figure 1), re-
ported by the authors in about 30-50% of cases.
5,19,20
Cury
et al.
3
found a prevalence of 19.6%, a result that may be
justified by the fact that the study was conducted in chil-
dren only. In addition, about 10-20% of patients will de-
velop proliferative retinopathy,
8
mainly in the fourth and
fifth decades of life.
21
D
iagnosis
In the early stages, the disease is asymptomatic, and me-
ticulous ophthalmologic monitoring should be performed.
8
Diagnosis is made by retinography and fluorescein angi-
ography in cases with fundoscopic alterations, as well as
measurement of visual acuity and intraocular pressure.
5,7,8,13
T
reatment
Treatment is performed in different ways, including dia-
thermy, cryotherapy and argon or xenon photocoagulation.
FIGURE 1
Increased vascular tortuosity.
1
FIGURE 2
“Black sunburst.”
1