














 14 / 113
14 / 113

S
alomão
R
et
al
.
564
R
ev
A
ssoc
M
ed
B
ras
2017; 63(7):564-565
IMAGE IN MEDICINE
Foix-Alajouanine syndrome mimicking a spinal cord tumor
R
enan
S
alomão
1
*, N
athalie
H
enriques
S
ilva
C
anêdo
2
, G
uilherme
P. A
brão
3
, C
arlos
L
ima
1
, M
arcus
A
ndré
A
cioly
1,4
1
Division of Neurosurgery, Universidade Federal do Rio de Janeiro (UFRJ), Rio de Janeiro, RJ, Brazil
2
Division of Neuropathology, UFRJ, Rio de Janeiro, Brazil
3
Division of Neuroradiology, Universidade Federal Fluminense (UFF), Niterói, RJ, Brazil
4
Division of Neurosurgery, UFF, Niterói, RJ, Brazil
S
ummary
Study conducted at the Department of
Neurosurgery, Hospital Universitário
Clementino Fraga Filho (HUCFF),
Universidade Federal do Rio de Janeiro
(UFRJ), Rio de Janeiro, RJ, Brazil
Article received:
11/8/2016
Accepted for publication:
1/3/2017
*Correspondence:
Hospital Universitário Clementino Fraga
Filho (HUCFF)
Address: Rua Rodolpho Paulo Rocco, 255
Rio de Janeiro, RJ – Brazil
Postal code: 21941-213
renansalomao_@hotmail.com http://dx.doi.org/10.1590/1806-9282.63.07.564Subacute necrotizing myelopathy (SNM) or Foix-Alajouanine syndrome is a
rare disease characterized by progressive neurological dysfunction caused by
a spinal dural arteriovenous fistula (AVF). Radiological diagnosis is usually
suspected when there is intramedullary nonspecific enhancement and peri-
medullary flow voids. Ring-enhancement is rarely reported in the scope of AVF,
which poses a diagnostic challenge and raises the suspicion of a spinal cord
tumor. In such situations, biopsy can be required and delay proper diagnosis.
We report the case of a patient with SNM, who underwent biopsy on the as-
sumption of it being a spinal cord tumor.
Keywords:
dural arteriovenous fistula, Foix-Alajouanine syndrome, spinal cord
glioma, subacute necrotizing myelopathy.
Subacute necrotizing myelopathy (SNM) is an uncommon
disease characterized clinically by progressive neurologi-
cal dysfunction.
1,2
In most of the patients, it is caused by
a spinal dural arteriovenous fistula (dAVF), also known
as Foix-Alajouanine syndrome.
1,3
dAVF leads to spinal
venous hypertension and infarction, as the pathological
end-stage of the disease.
1
Such acute/subacute deteriora-
tion occurs in 14.8% of the patients.
4
This 71-year-old lady was admitted to our department
after suffering from a progressive neurological deterioration
of the lower limbs, as well as sphincter dysfunction over
the last two years. Five days before admission, the patient
was affected by severe lumbar pain, which was followed by
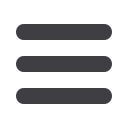
rapid severe paraparesis. Imaging revealed an expansive
lesion at D12-L1 with ring-enhancement and subtle peri-
medullary flow voids (Figure 1). The patient underwent
biopsy of the lesion, on the assumption of it being a spinal
cord tumor. Initially, it was misinterpreted as a high-grade
glioma on frozen specimens, but final histological analysis
revealed the typical findings of SNM. Superselective spinal
angiography confirmed dAVF diagnosis (Figure 1), and the
patient was taken to surgery for definitive treatment.
FIGURE 1
Sagittal T1- (A), T2- (B), and T1-weighted with gadolinium enhancement and fat suppression (C) showed diffuse fusiform
enlargement of the spinal cord up to the level of the conus medullaris together with ring-like enhancement at D12-L1. A subtle serpentine pattern
of flow voids was observed on T2-weighted images (B). In D, superselective angiogram in frontal view revealed enlarged vessels on the left side of
the spinal canal at the level of D12 (white arrow head), as well as the Adamkiewicz artery (black arrows) and the draining vein (white arrow).
A
B
C
D