














 14 / 105
14 / 105

M
onteiro
VB
et
al
.
734
R
ev
A
ssoc
M
ed
B
ras
2017; 63(9):733-735
ischemic heart disease. In the anatomopathological exam-
ination, the heart weighed 310 g and the heart weight to
body weight ratio was 0.57%. There had been a recent trans-
mural infarction measuring about 3 cm in length in the
lower third of the interventricular septum and anterior wall
of the left ventricle, with rupture of the septum and conse-
quent interventricular communication in the lower front
portion of the septum, measuring about 1 cm in diameter.
There was severe atherosclerosis in the left coronary artery
and its branches, especially in the anterior descending and
the circumflex branches, with a recent thrombus in the an-
terior descending artery. Passive hepatic congestion (weight
1,490 g) and renal congestion (right kidney weight 140 g; left
150 g) with atherosclerosis and degenerative phenomena in
the tubules were observed, as well as pulmonary (weight of
the right lung 480 g; left 400 g), encephalic (weight 1,000 g)
and inferior limb edema. Moderate atherosclerosis in the
aorta with atheroma and fibrous plaques was also observed.
Case 2: Male patient, 67 years, white, single, born in
Santa Juliana (Minas Gerais), residing in Uberaba (Minas
Gerais), agricultural worker, died on August 22, 1980. He
presented hypertensive and ischemic heart disease. There
had been a recent infarction with intracardiac thrombo-
sis, affecting the lower third of the interventricular septum
in its right half, apex of the left ventricle and right ven-
tricle, measuring in its largest diameters about 4.5 by 3.5
cm. Rupture in the apex of the right ventricle with 0.4 cm
in length and hemopericardium. Atherosclerosis was
found in the left coronary, especially in the front inter-
ventricular branch, calcification and recent thrombosis.
The lungs were edematous.
Case 3: Male patient, 67 years, white, married, born
in Ipiau (Bahia), residing in Uberaba (Minas Gerais), retired
carpenter, died on August 23, 2007. The patient had dia-
betes mellitus, was admitted to the emergency room in a
state suggesting non-controlled asthma or chronic ob-
structive lung disease. He died suddenly on the 4
th
day,
after lung function stabilization. On autopsy, hyperten-
sive heart disease and ischemic heart disease were verified.
There was global hypertrophy of the myocardium, espe-
cially in the left ventricle, with cardiac weight of 470 g
and the heart weight to body weight ratio was 0.71%. A
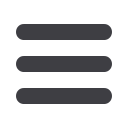
recent infarction was observed, in accordance with the
upper-posterior region of the left ventricle, next to the
coronary circumflex artery, measuring about 2.0 by 1.0 cm,
with a recent rupture of 0.5 cm, and consecutive hemoperi-
cardium (Figure 1). There was marked atherosclerosis of
the aorta, especially of the thoracic portion and its main
branches. The lungs presented edema and congestion
(right lung 435 g; left 494 g).
D
iscussion
Our study includes all the cases of autopsied patients in
the last 30 years, during the period from 1979 to 2009,
with a diagnosis of cardiac rupture as a result of a recent,
acute myocardial infarction. In this period, the percentage
of AMI with rupture of the myocardium was 0.2%.
Risk factors for rupture of the myocardium post-AMI
include older age, diabetes mellitus and systemic arte-
rial hypertension. In only one case, that of the patient
who developed interventricular communication, there
was doubt regarding the pre-death diagnosis. Rupture
of the right ventricle with hemopericardium is also rare,
and, to our knowledge, has never been reported in a series
of cases.
5,6
Ventricular rupture post-AMI occurs in 1 to 4% of
cases, and is responsible for about 5% of premature deaths
after acute myocardial infarction.
1
Strong suspicion and
confirmation by means of echocardiography are import-
ant for the diagnosis and eventual surgical intervention,
which is currently the only way of treating this condition.
4-6
Although there is a worldwide trend of a lower num-
ber of autopsies, this diagnostic method continues to be
important as a form of quality control of the clinical di-
agnosis made while the patient is alive, and the verification
of the agreement of the methods. Autopsies are not only
important for medical teaching, but may also help to
elucidate unexpected deaths, including those of hospital-
ized patients, as in the case of our series.
FIGURE 1
Case 3: Heart with a recent infarction corresponding
to the upper-posterior area of the left ventricle and a recent rupture
of 0.5 cm.