













 93 / 102
93 / 102

L
ocal
management
with
methotrexate
of
cesarean
scar
ectopic
pregnancy
with
live
embryo
guided
by
transvaginal
ultrasound
: A
case
report
R
ev
A
ssoc
M
ed
B
ras
2016; 62(2):184-187
187
peated when
β
-hCG reaches a negative value or after 3
months of drug treatment. This should only be brought
forward if there are new episodes of bleeding.
In our case, a surgical approach was not required,
using merely drug treatment with a local dose plus three
local doses of systemic methotrexate. However, a slow re-
gression of
β
-hCG values was observed to the initially
high values, taking 58 days to reach negative values. An
Australian article about 13 cases of cesarean scar ecto-
pic pregnancy suggests that the association of local drug
treatment with systemic doses can reduce the time in-
terval for
β
-hCG to become negative and that local meth-
otrexate seems to be more effective than systemic treat-
ment alone due to the presence of fibrotic tissue in the
region of the scar, limiting the access of systemic medi-
cation.
14
After 3 to 6 months of disappearance of the image of
the ectopic pregnancy, our recommendation is to per-
form hysterosalpingography and hysteroscopy for better
assessment of the uterine cavity, as well as adequate re-
productive planning for these patients.
C
onclusion
The early diagnosis of cesarean scar ectopic pregnancy is
performed via transvaginal ultrasound and is fundamen-
tal for the indication of suitable conservative treatment.
Drug treatment with a local dose of ultrasound-guided
methotrexate in the presence of a live embryo, associat-
ed with a protocol of multiple doses of systemic metho-
trexate when
β
-hCG exceeds 5,000 mIU/mL has been
found effective, preventing mutilating surgeries and spar-
ing fertility in these patients.
R
esumo
Tratamento local com metotrexato guiado por ultrasso-
nografia transvaginal de gravidez ectópica em cicatriz de
cesárea com embrião vivo: relato de caso
A gravidez ectópica na cicatriz de cesárea é uma forma rara
de gestação ectópica com elevada morbimortalidade. O em-
prego de condutas conservadoras, como o tratamento me-
dicamentoso commetotrexato, tem evitado cirurgias muti-
ladoras, como a histerectomia, e preservado o futuro
reprodutivo da mulher. Relatamos um caso de paciente de
30 anos, com gravidez ectópica em cicatriz de cesárea, com
embrião vivo, tratada com injeção local de metotrexato guia-
da por ultrassonografia transvaginal, complementada com
tratamento sistêmico commúltiplas doses de metotrexato.
Palavras-chave:
gravidez ectópica, metotrexato, cicatriz,
cesárea.
R
eferences
1.
Fylstra DL, Pound-Chang T, Miller MG, Cooper A, Miler KM. Ectopic
pregnancy within a cesarean delivery scar: a case report. Am J Obstet Gynecol.
2002; 187(2):302-4.
2.
Jourdain O, Fontanges M, Schiano A, Rauch F, Gonnet JM. [Management
of other ectopic pregnancies (corneal, interstitial, angular, ovarian)]. J Gynecol
Obstet Biol Reprod (Paris). 2003; 32(7 Suppl):S93-100.
3. Bignardi T, Condous G. Transrectal ultrasound-guided surgical evacuation of
cesarean scar ectopic pregnancy. UltrasoundObstet Gynecol. 2010; 35(4):481-5.
4.
Jurkovic D, Hillaby K, Woelfer B, Lawrence A, Salim R, Elson CJ. First-
trimester diagnosis and management of pregnancies implanted into the
lower uterine segment Cesarean section scar. Ultrassond Obst Gynecol.
2003; 21(3):220-7.
5. SeawKM,HuangLW,linYH,LinMY,TsaiYL,HwangJL.Cesareanscarpregnancy:
issues inmanagement. UltrassoundObstet Gynecol. 2004; 23(3):247-53.
6.
Herman A, Weinraub Z, Avrech O, Maymon R, Ron-El R, Bukovsky Y. Follow
up and outcome of isthmic pregnancy located in a previous caesarean section
scar. Br J Obstet Gynaecol. 1995; 102(10):839-41.
7. Vial Y, Petignat P, Hohlfeld P. Pregnancy in a cesarean scar. Ultrasound
Obstet Gynecol. 2000; 16(6):592-3.
8. Rotas MA, Haberman S, Levgur M. Cesarean scar ectopic pregnancies: etiology,
diagnosis, and management. Obstet Gynecol. 2006; 107(6):1373-81.
9. Larsen JV, SolomonMH. Pregnancy in a uterine scar sacculus – an unusual cause
of postabortal haemorrhage. A case report. S Afr Med J. 1978; 53(4):142-3.
10. Timor-Tritsch IE, Monteagudo A. Unforeseen consequences of the increasing
rate of cesarean deliveries: early placenta accreta and cesarean scar pregnancy.
A review. Am J Obstet Gynecol. 2012; 207(1):14-29.
11. Agarwal N, Shahid A, Odejinmi F. Caesarean scar pregnancy (CSP): a rare
case of complete scar dehiscence due to scar ectopic pregnancy and its
management. Arch Gynecol Obstet. 2013; 288(1):231-2.
12. Ash A, Smith A, Maxwell D. Caesarean scar pregnancy. BJOG. 2007;
114(3):253-63.
13.
Fylstra DL. Ectopic pregnancy within a cesarean scar: a review. Obst Gynecol
Surv. 2002; 57(8):537-43.
14.
Michener C, Dickinson JE. Caesarean scar ectopic pregnancy: a single centre
case series. Aust N Z J Obstet Gynaecol. 2009; 49(5):451-5.
15.
Elito J, Araujo E, Santana EFM, Szejnfeld D, Helfer TM, Nardozza LMM, et
al. Uterine artery embolization with methotrexate infusion as treatment for
cesarean scar pregnancy. Med Ultrason. 2013; 15(3):240-3.
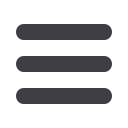
FIGURE 3
Transvaginal ultrasonography after 3 months of drug
treatment with local and systemic methotrexate for cesarean scar
ectopic pregnancy.