













 91 / 102
91 / 102

L
ocal
management
with
methotrexate
of
cesarean
scar
ectopic
pregnancy
with
live
embryo
guided
by
transvaginal
ultrasound
: A
case
report
R
ev
A
ssoc
M
ed
B
ras
2016; 62(2):184-187
185
than 5,000 mIU/mL, and a single dose if less than 5,000
mIU/mL; drug treatment with local injection of metho-
trexate guided by transvaginal ultrasound if the embryo
is alive, with an association made with the protocol for
multiple dose of systemic methotrexate if the
β
-hCG val-
ue exceeds 5,000 mIU/mL. In the last treatment option,
methotrexate is given at a dose of 1 mg/kg, initially with
local injection, followed by 3 intramuscular doses on al-
ternate days. In the days between these doses, folinic acid
was administered at a dose of 0.1 mg/kg and control tests
for possible methotrexate toxicity (hepatic and renal func-
tion), and
β
-hCG dosage are measured.
In this case report the patient presented a cesarean
scar ectopic pregnancy with live embryo and
β
-hCG of
18,716 mIU/mL. As such, local treatment with transvag-
inal ultrasound-guided injection of methotrexate was in-
dicated, complemented with the protocol of multiple sys-
temic doses of methotrexate.
Post treatment follow-up was done with weekly dos-
ing of
β
-hCG up to a value of less than 5,000 mIU/mL
and realization of transvaginal ultrasound until the ab-
sence of the Doppler flow.
C
ase
report
The 30-year old pregnant patient, weighing 68 kg,
secundi-
gravida
, with previous cesarean delivery 12 years before, was
6 weeks late on her period although presenting a small
amount of vaginal bleeding for 1 day. On physical exami-
nation the patient was hemodynamically stable; in the spec-
ulum examination there was the presence of vaginal bleed-
ing collected in small quantities; and in the touch
examination the cervix was impervious, with an increased
uterus for 6 weeks, and palpable attachments without chang-
es. The laboratory tests were:
β
-hCG of 18,716, mIU/mL,
blood test with hemoglobin (Hb) of 12.8 g/dL, hematocrin
(Ht) of 38.5%, leukocytes of 7,450/uL, platelets of 209,000/
uL, positive O Rh blood typing, 0.57 mg/dL of creatinine,
urea of 18 mg/dL, SGOT of 26 U/L and SGPT of 28 U/L.
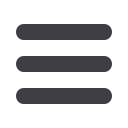
Transvaginal ultrasound performed on this day showed
a 6 mm crown to rump length (CRL), corresponding to
gestational age of 6 weeks and 4 days, a gestational sac of
16 x 14 x 9.6 mm located at the site of the previous cesare-
an section scar with a live embryo (126 bpm fetal heart
rate), an empty uterine cavity and attachments without
changes. The gestational sac was located approximately 22
mm from the external orifice of the cervix (Figure 1).
Due to the presence of the live embryo, the patient
was submitted to transvaginal ultrasound-guided punc-
ture and injection of methotrexate inside the gestation-
al sac at 68 mg (1 mg/kg). A 17 Gauge Cook
®
Medical
needle was used, guided by the Aloka 500
®
ultrasound
apparatus.
In addition to the local dose, three 68 mg intramus-
cular doses of methotrexate (1 mg/kg) interspersed with
4 intramuscular doses of folinic acid at 6.8 mg (0.1 mg/
kg) were given.
The patient remained in hospital until the last dose
of folinic acid without clinical complications after the
procedure, showing only slight abdominal colic treated
with analgesia, receiving a discharge with weekly follow-
up at the outpatient clinic specializing in ectopic preg-
nancy at Hospital São Paulo (Unifesp).
It is important to note that blood test, hepatic and
renal function examinations remained normal from ad-
mission to discharge from hospital.
Seven days after discharge, the patient sought the
Gynecology and Obstetrics emergency service of the Hos-
pital São Paulo complaining of vaginal bleeding. In the
physical examination the patient was found to be hemo-
dynamically stable, the abdominal examination showed
no changes, the specular examination showed the pres-
ence of a discrete amount of blood collected, painless vag-
inal touch with impervious cervix, and intrapelvic uter-
us and attachments normal to the touch. The laboratory
examinations on this occasion were still normal (blood,
hepatic and renal function), showing that there was no
methotrexate toxicity, with Hb of 12 g/dL and
β
-hCG of
6,129 mIU/mL. Another ultrasound examination was per-
formed with uterine volume of 200 cm³ and presence of
a cystic image on the anterior uterine wall with anecho-
ic content and irregular walls, measuring 1.3 x 1.2 x 0.5 cm,
without characterization of an embryo, endometrial echo
of 1.2 cm and unchanged attachments.
FIGURE 1
Ultrasonography showing the anatomical relationship
between bladder, cervix, uterine body and gestational sac in the
topography of the cesarean scar, with an empty uterine cavity.