













 38 / 105
38 / 105

S
ilva
SA
da
et
al
.
228
R
ev
A
ssoc
M
ed
B
ras
2016; 62(3):227-230
nopathy and lesions in target organs (liver, kidneys, lungs,
brain, muscles, thyroid, pancreas, heart), DRESS syn-
drome is a rare example of life threatening drug hyper-
sensitivity reaction.
1-3
The incidence of this syndrome is unknown. The fre-
quency varies depending on the drug used and the im-
mune status of the individual.
2
The period from drug exposure to onset of disease
can last 2 to 6 weeks, and may persist with a series of re-
missions and relapses. After discontinuation of the drug,
the average recovery time is 6-9 weeks. DRESS syndrome
has an approximate mortality rate of 10%.
2-4
Predictors
of poor prognosis have not been identified so far, but pa-
tients with increased liver impairment and advanced age
are at increased risk of death.
2,5
There are reports of cas-
es of autoimmune disease months to years after the res-
olution of the syndrome.
6
Given that this is a rare but severe disease, we report
a case of DRESS syndrome in a 20-year old female pa-
tient, black, former alcoholic and former user of cocaine,
with epilepsy and non-specified neuropsychiatric disor-
der, admitted to Hospital Municipal Odilon Behrens
(HMOB), Belo Horizonte, state of Minas Gerais, present-
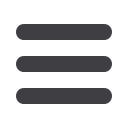
ing fever of 38ºC, prostration and drowsiness. After two
days of onset of symptoms, the patient developed jaun-
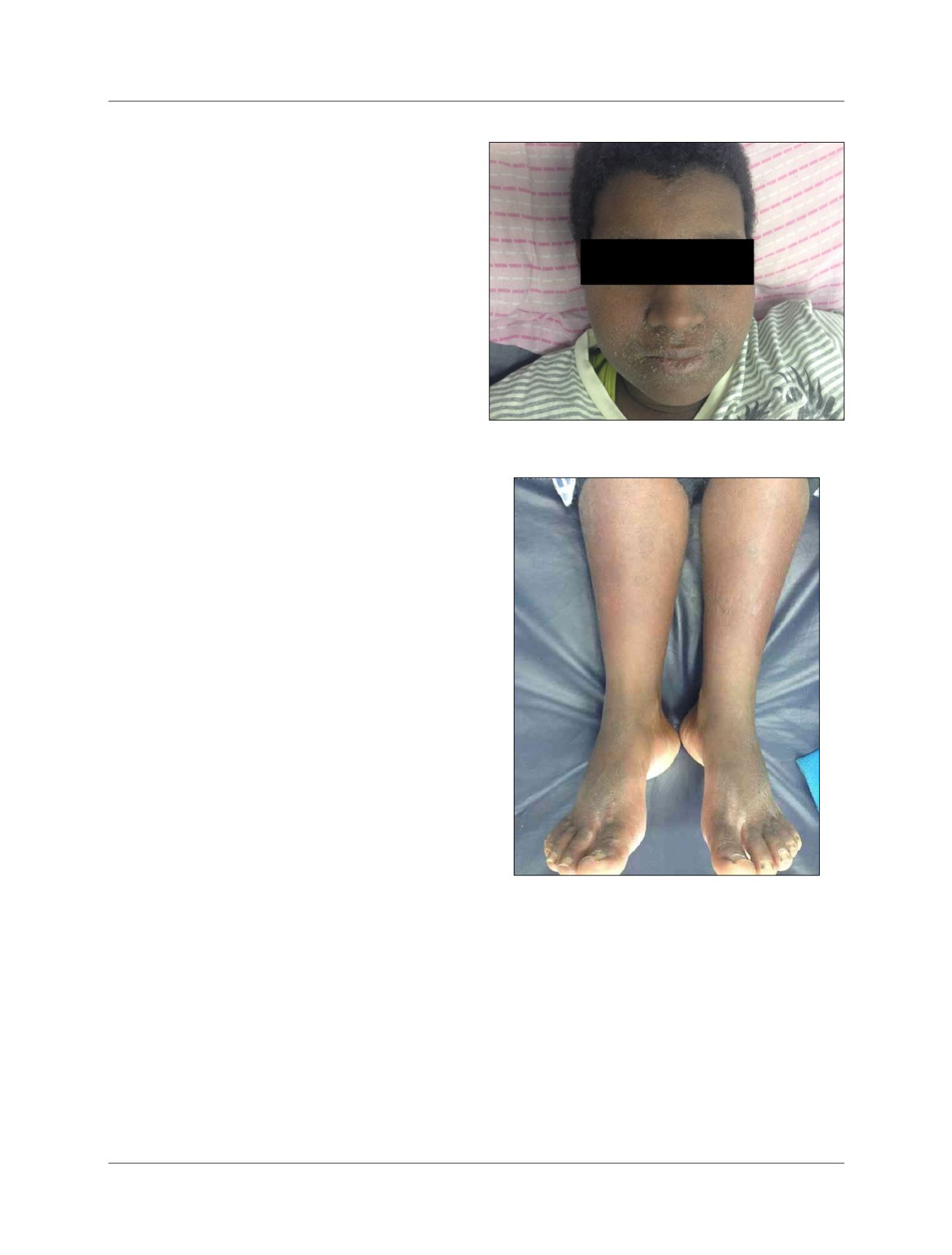
dice (+/4), bipalpebral and lower limbs edema (++/4), mac-
ular erythema and lamellar desquamation in the face,
trunk, upper and lower extremities (Figures 1 and 2) and
bilateral cervical lymph node enlargement, with approx-
imately 1 cm in diameter, painless and mobile. The pa-
tient had been undergoing irregular home treatment
with diazepam, haloperidol and valproic acid for 4 weeks.
Initially, the symptoms were treated as soft tissue infec-
tion with prescription clavulanate amoxicillin and
azithromycin, suspended on hospital admission.
Laboratory tests performed on admission showed
normocytic and normochromic anemia, thrombocyto-
penia, leukocytosis without a left shift and with mild
neutropenia, atypical lymphocytosis and eosinophilia
(9%; 973/mm
3
), as well as elevated levels of C-reactive pro-
tein (CRP), transaminases (2 times the reference value),
alkaline phosphatase (ALP), gamma-glutamyl transpep-
tidase (GGT), bilirubin (direct and indirect) and chang-
es in kidney function. Serology for human immunode-
ficiency virus and hepatitis B and C were negative. Chest
radiography revealed no abnormalities, while abdomi-
nal ultrasound showed mild hepatomegaly and contract-
ed gallbladder.
In view of a possible diagnosis of DRESS syndrome,
the patient was hospitalized and corticosteroid therapy
with prednisone (40 mg once daily) was initiated. The drugs
that the patient used at home (valproic acid and haloper-
idol) were suspended, and only diazepam was continued.
After ten days of the introduction of corticosteroid
therapy, the patient progressed asymptomatic, afebrile,
with progressive improvement of skin lesions, even though
a scaly appearance continued. The dosage of liver trans-
aminases, ALP, GGT, bilirubin, CRP, lymphocytes and
eosinophils remained high, although lower than those at
admission. There was improvement in kidney function.
FIGURE 1
Diffuse desquamative erythema and face edema.
FIGURE 2
Diffuse erythema and edema in the lower limbs.