













 44 / 105
44 / 105

C
osta
and
H
yeda
234
R
ev
A
ssoc
M
ed
B
ras
2016; 62(3):231-235
630.51-696.49). There was an absolute reduction of 79%
in days of hospitalization in the CDMCP group compared
to the other group.
The total health care costs of the selected users were
divided by gender, age group and ICD-10. In the CDMCP
group, women accounted for 48% (BRL 15,227,379.12),
while male users were 52% (BRL 16,248,274.60) of the to-
tal cost of the program (BRL 31,475,653.72). That is, there
was no significant statistical difference in health care costs
between females and males (SD±BRL13,014.84, 95CI
BRL13,086.34-BRL14,525.88). The greatest concentration
of health care costs in the CDMCP group (51%) was in the
age group of 50 to 70 years (BRL 16,121,060.53) with a cost
per patient of BRL 24,397.42. Cardiovascular diseases and
neoplasms accounted for the greatest health care cost in
the CDMCP group (64%), with the cost per user classified
as having a neoplasm at BRL 46,176.39 and cardiovascu-
lar diseases at BRL 24,536.40. CDMCP participants with
health insurance (786) were responsible for 60% of the costs
of the program (BRL 18,906,794.34) with the cost per pa-
tient with insurance at BRL 24,054.45 and per dependent
patient at BRL 26,742.25.
The total cost of the CDMCP group in the period of
20 months was BRL 31,475,653.72 corresponding to
68.06% of the cost of patients in the non-CDMCP group
(BRL 46,245,735.84). Despite the lack of statistical sig-
nificance, the CDMCP contributed to an absolute reduc-
tion of 31.94% in total health care costs, with an 8.63%
reduction in monthly costs, and a total reduction of BRL
40,529,349.28 (Table 2).
D
iscussion
In our analysis, we observed that the distribution of
CDNCD patients with severe characteristics (frequent hos-
pitalizations and/or emergency consultations in the year
preceding the CDMCP) and that needed CDMCP care was
similar between genders and had a predominance of indi-
viduals aged over 50 years. These results are in accordance
with the literature,
5,13-16,18
which shows the similarity of the
data studied in relation to the actual world population.
It is important to note that patients with a CDNCD are
a heterogeneous population, with different medical care
needs: 70-80% need only support and education for self-
management of their pathology, while a minority needs in-
tensive hospital care. CDNCD patients, without proper
monitoring or not adhering to treatment, have a high risk
of complications, poorer quality of life and greater spend-
ing with high cost procedures in health systems.
13,18
In the
population studied, an absolute reduction was observed in
number of days of hospitalizations (79%) compared to us-
ers who had the same clinical conditions and chose not to
participate in the program. The lack of individual monitor-
ing of the population in the CDMCP groupmay be related
to a higher number of hospitalizations and, possibly, low-
er adherence to non-pharmacological treatment measures.
The cost reduction observed was relevant: a 31.94%
reduction in the total costs and 8.63% reduction in month-
ly costs, considering that the program evaluated in this
study only offered verbal guidance to users, encouraging
self-management of pathologies by patients, without in-
terfering with the treatment plan established by the at-
tending physician (in accordance with the fundamental
elements of the programs based on the Chronic Care
Model – CCM
17,18
).
In the same context, the ANS has established stan-
dards for Supplementary Health Plans in Brazil to offer
users programs for chronic disease management, under
Normative Resolutions No. 264 and 265.
14
As noted in this
study, it is possible to apply the CDMCP in the supplemen-
tary health sector, not only in the public system, with health
care quality benefits and overall cost reduction.
In the context of Clinical Governance for continuous
improvement of the quality in health care,
19
the CDMCP
analyzed in this study incorporated a focus on the individ-
ual and on health promotion for those being monitored
by it. The health care provided by the case manager (ob-
served in this study) including guidance and information
for self-management of chronic pathologies respects the
principles of clinical governance of completeness and fair-
ness of the care, respecting the patient’s autonomy.
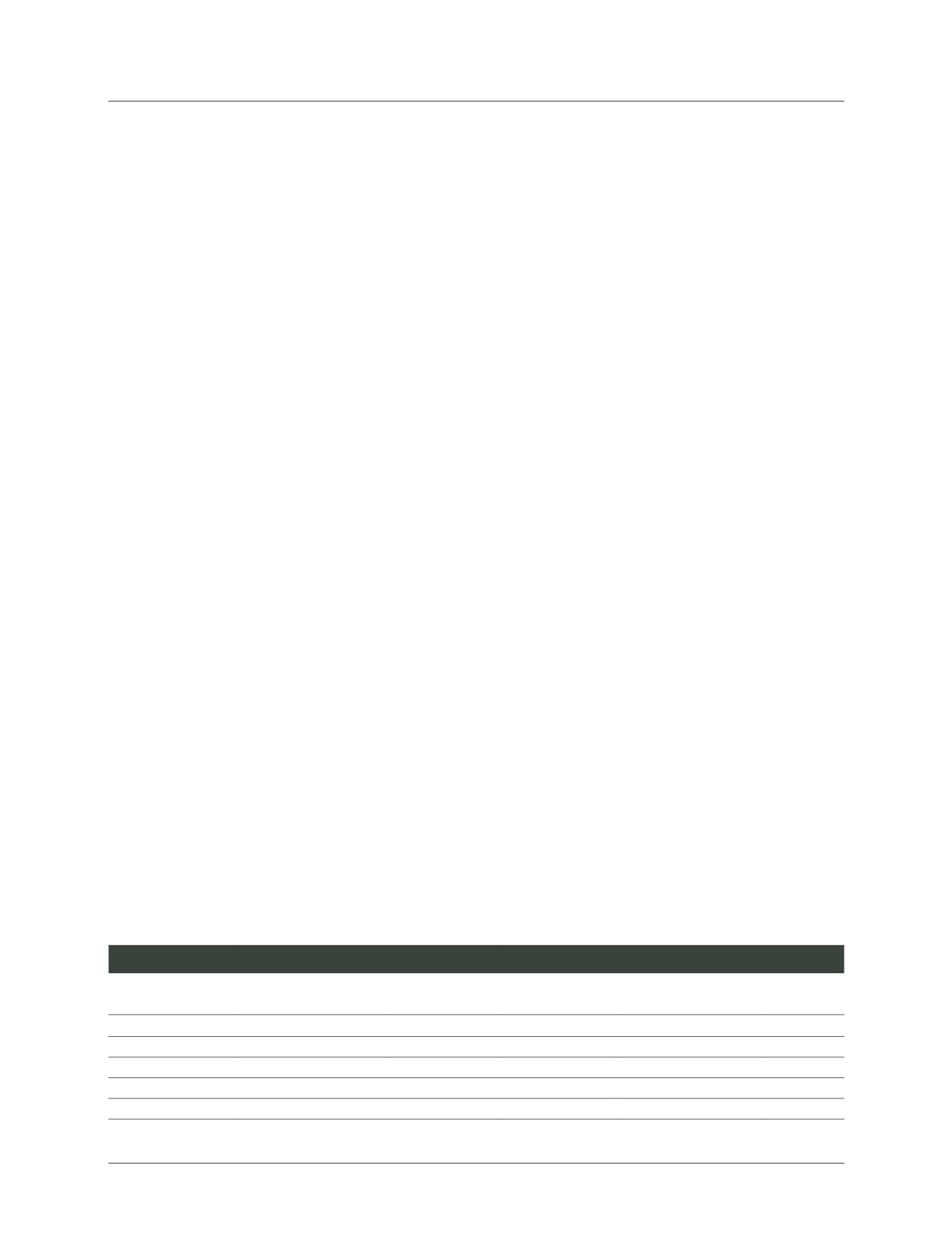
TABLE 2
Clinical and demographic characteristics of the CDMCP and non-CDMCP groups.
Characteristics
CDMCP group
Non-CDMCP
group
(n=1256)
(n=851)
Mean
Standard deviation (±) 95CI
Women
639
379
509.00
183.848
11.2936
Men
617
472
544.50
102.530
6.0896
Hospitalization (days) 230
1097
663.50
613.062
32.9850
Cost (BRL)
BRL31,475,653.72
BRL46,245,735.84 BRL38,860,694.78 BRL10,444,025.23
BRL2,321.91
CDMCP: chronic disease management care programs.