













 90 / 99
90 / 99

W
ong
A
et
al
.
470
R
ev
A
ssoc
M
ed
B
ras
2016; 62(5):468-473
possible causative agents. Carcinomas and lymphomas are
also associated. Notwithstanding the different known eti-
ologies, SJS is idiopathic in 25 to 50% of cases.
1,7
C
linical
picture
For most drugs triggering these reactions, there is an inter-
val ranging from4 to 28 days between the beginning of drug
use and the onset of signs and symptoms. The highest risk
of developing SJS and TEN occurs in the first 2 months of
treatment with risk drugs on a continuous basis.
Both diseases can start with prodromal symptoms
lasting up to 1 week, such as fever, sore throat, coughing,
eye burning, myalgia and arthralgia. After this period
there may be a discrete maculopapular rash, similar to a
morbilliform rash.
1,4
There may be atypical target lesions (with two instead
of the three characteristic concentric rings found in EM)
on the back of the hands, palms, sole of the foot, exten-
sor surface of the limbs, neck, face, ears and perineum,
with prominent involvement of trunk and face.
1,4
The rash begins on the trunk with subsequent gener-
alization, usually sparing the palmoplantar areas. Macu-
lar lesions become purplish, and epidermal detachment
occurs, resulting in flaccid blisters that converge and break,
resulting in extensive sloughing of necrotic skin (Figure 1).
Nikolsky’s sign is positive in perilesional skin.
1
The difference between SJS and TEN would be the
percentage of affected body area: cases involving less than
10% of the body would be classified as SJS, and those with
over 30% of involvement would be TEN. Cases with in-
volvement between 10 and 30% would be considered a su-
perposition of the two entities.
4
Mucosal involvement occurs in two or more distinct
mucosal surfaces and may precede or follow the skin in-
volvement. It begins with enanthem and edema that cause
erosions and pseudomembranous formations in the eyes,
mouth, genitals, throat and upper airways. About 10-30%
of cases occur with fever and lesions in the gastrointesti-
nal and respiratory tracts.
4
Ocular involvement may be present in 39 to 61% of
the cases presenting complications such as corneal ulcer,
anterior uveitis, and panophthalmitis. Gastrointestinal
adhesions, urinary incontinence, vaginal stenosis, renal
tubular necrosis, renal failure, skin ulcerations with re-
infection and non-esthetic scars are not uncommon.
7
Loss of integrity of the skin barrier leads to increased
chance of secondary bacterial infection, as well as distur-
bances in electrolyte balance and thermoregulation.
1
L
aboratory
testing
There are no laboratory tests to point out the drug caus-
ing the disorder and, therefore, diagnosis is clinical.
13
A
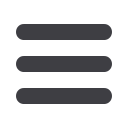
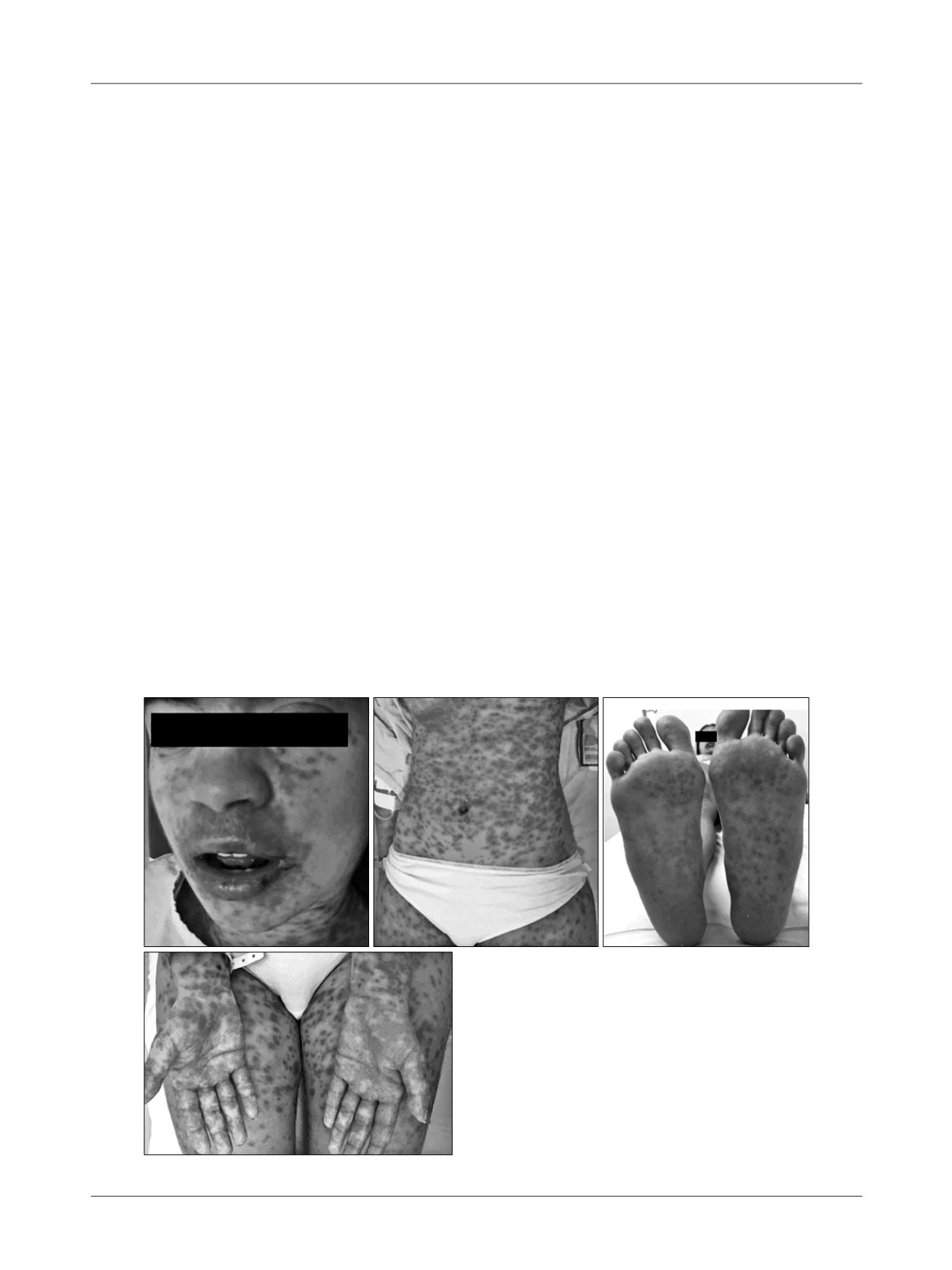
FIGURE 1
Patient with Stevens-Johnson syndrome, 5 days after
the use of piroxicam. Courtesy: Dr. Karine Simone, Internal
Medicine outpatient clinic, Dermatology, Santa Casa de São Paulo.