














 61 / 70
61 / 70

M
olina
J
unior
WR
et
al
.
718
R
ev
A
ssoc
M
ed
B
ras
2017; 63(8):717-721
databases to identify relevant studies. Six separate search-
es were done by applying the following free-text search
terms: “Safety guidewire ureteroscopy,” “Safety guidewire
flexible ureteroscopy,” “Safety wire ureteroscopy,” “Safe-
ty wire retrograde intrarenal surgery” and “Safety wire
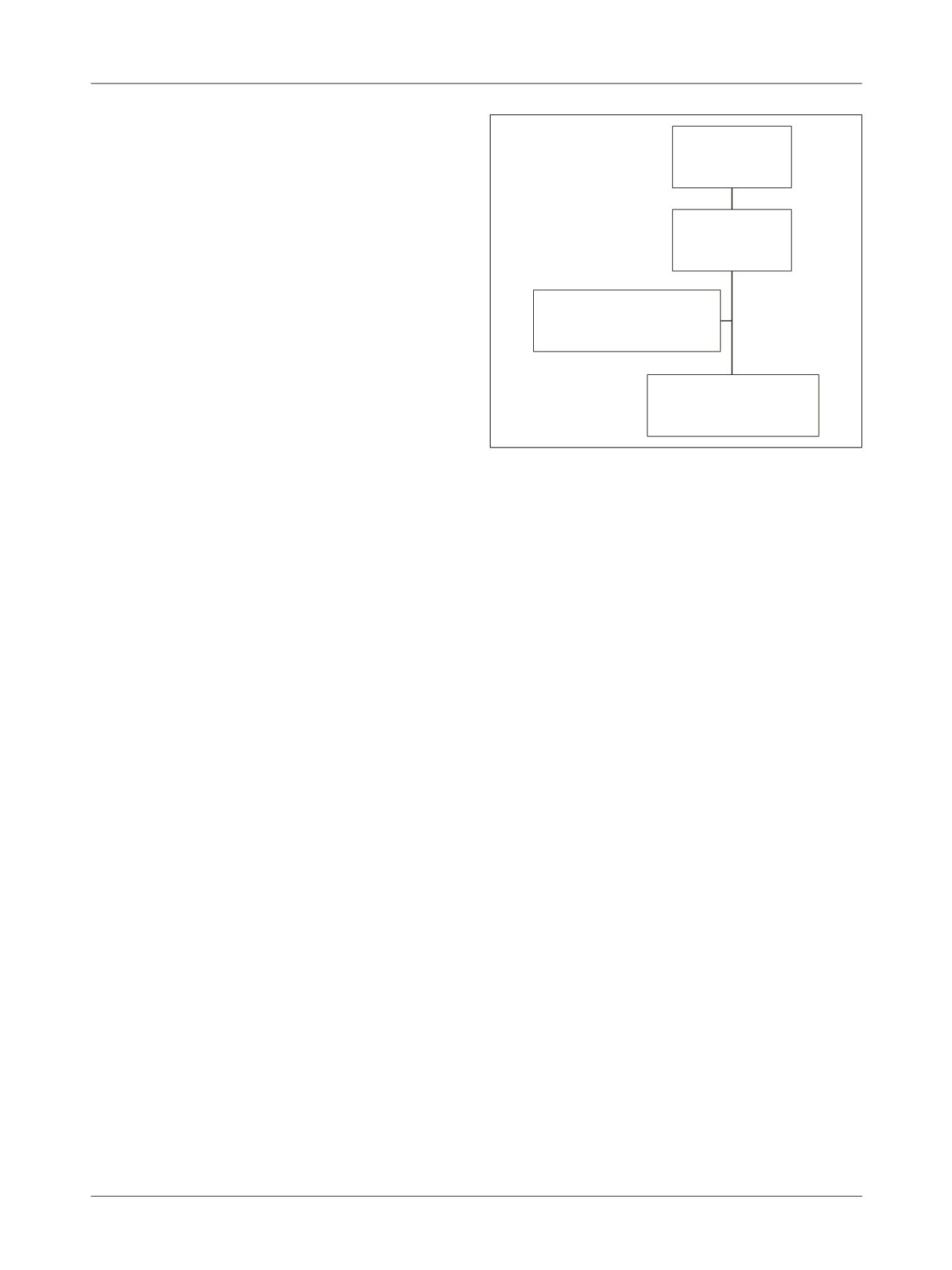
upper ureter.” Article selection was done based on Pre-
ferred Reporting Items for Systematic Reviews and Meta-
-Analyses (PRISMA) criteria
7
(Figure 1). Titles of articles
were first reviewed to determine whether they might fit
the inclusion criteria. After assessing the abstract, a more
detailed subsequent assessment was performed by look-
ing at the full text. References of included studies were
also reviewed to identify additional studies of interest.
Two reviewers (R.P and W.M) independently screened
all the titles and abstracts to minimize selection bias. The
quality of the evidence was evaluated based on compre-
hensiveness of the data and precision of the reporting
according to the criteria provided by the Centre for Evi-
dence-Based Medicine in Oxford, UK (website, same 18
as Cryometa). Only studies where an SGW was both used
and omitted in the same cohort of patients were includ-
ed. The initial literature search identified 72 potentially
relevant studies. Their titles and abstracts were screened
for relevance, resulting in 44 potential articles after ex-
cluding duplicate results. Four reports were excluded
because they were review URS articles and 35 were ex-
cluded because they didn’t specifically addressed the use
or not of an SGW. Therefore, five articles were included
and one additional record was added after reference list
survey (Figure 1). The primary outcome was to report
feasibility, contraindications to and complications of
performing intrarenal retrograde flexible and semi-rigid
URS without the use of an SGW. Secondary outcomes
were to compare stone-free rates and complications be-
tween cases where an SGW was used or omitted for the
treatment of ureteral and kidney stone disease. Patients
were considered stone-free if they had remnant fragments
of up to 2 mm in follow-up tomography or intravenous
urography six weeks to three months after the main pro-
cedure. The Clavien-Dindo classification was used to
report complication.
8
R
esults
Six studies (Table 1) were identified and selected for this
review. Overall, they included 1,886 patients, and either
semi-rigid or flexible URS was performed without the use
of an SGW for the treatment of urinary calculi disease.
Four of them were retrospective observational non-com-
parative studies (level of evidence 4)
6,9-11
and two were
retrospective observational non-consecutive comparative
studies (level of evidence 3b).
4,11
Johnson et al.
10
studied retrospectively a single-sur-
geon prospective database of flexible URS. A total of 186
patients were submitted to wireless flexible URS for the
treatment of intrarenal stones. They reported a stone-free
rate of 90, 89 and 75% after primary therapy of intra-renal
calculi of < 1.0 cm, 1.0 to 2.0 cm, and > 2.0 cm, respec-
tively. Stone-free rates after primary treatment of ure-
teral calculi were 93, 96 and 100% for proximal, medial
and distal third location, respectively. Inability to access
the lower pole was reported in six cases and inability to
reach the kidney, in one. There were no false passages or
ureteral perforations secondary to endoscope placement.
Minor complications were limited to postoperative py-
elonephritis in five individuals and gross hematuria in
three, both treated successfully with antibiotics and with
conservative measures, respectively.
10
Dickstein et al.
6
reported their experience with flex-
ible URS for the treatment of ureteropelvic junction (54)
and renal calyces (216) stones in 270 consecutive patients.
In all cases, lithotripsy was performed with a Holmium:YAG
laser until calculi pulverization, without the use of a
basket for extraction of fragments. The average stone
size was 9.1±3.5 mm, and stone-free rate was 88.9% (240
of 270). There were no intraoperative complications, no
cases of lost access, ureteral perforation, avulsion, or the
need for a percutaneous nephrostomy tube placement
(PCNT). However, the authors still recommended the
use of an SGW in cases of complicated cases, such as
encrusted ureteral stents, ureteral stricture requiring
Articles after
duplicates removed:
44 papers
38 excluded: 4 review articles;
non-related to safety guidewire
in ureteroscopy 34 articles
Six papers included
addressing the use of a safety
wire during ureteroscopy
Articles screened
based on title and
abstracts: 44
FIGURE 1
Paper selection.