













 17 / 102
17 / 102

Z
ika
virus
infection
and
pregnancy
R
ev
A
ssoc
M
ed
B
ras
2016; 62(2):108-115
111
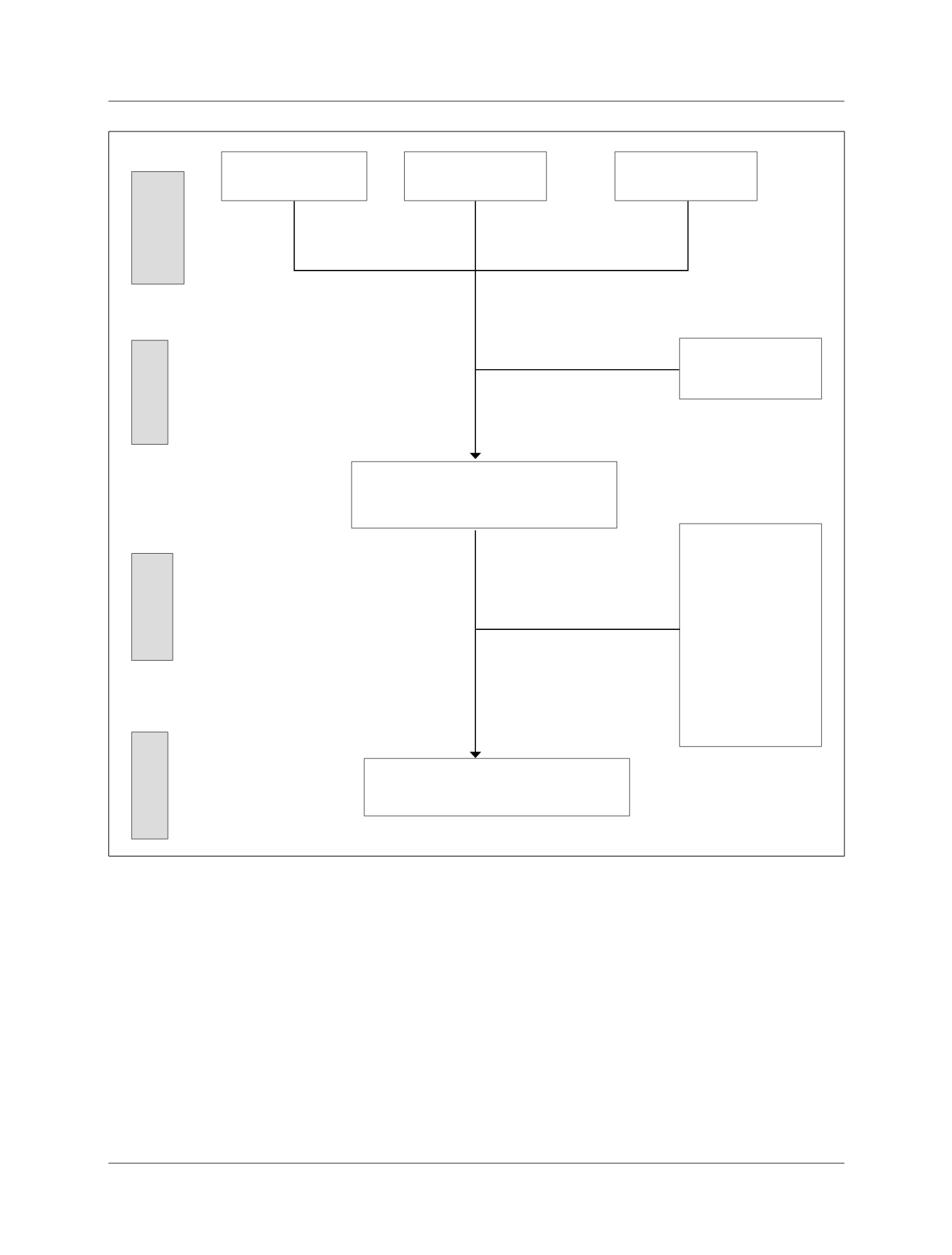
FIGURE 1
Flowchart for study selection.
Search
Eligibility
Included
Articles selected to be included in the guideline
n=30
Search
identification
Pubmed/Medline
n=173
Embase
n=171
Articles selected for detailed reading of the full
text n=288
Studies excluded
because they were not
related to the
components of P.I.C.O.
(n=171); physiological
studies or animal
models (n=46); lack of
full text (n=41)
Duplicate articles n=56
Cochrane
n=0
vous system in Brazil, which is about five cases per 100,000
live births, less than the estimates recently made of 10 to
20 cases per 100,000 live births. This may indicate the oc-
currence of underreporting of microcephaly in the
country.
18
(
D
) Thus, any active search for this congenital
malformation would be able to increase its prevalence, with
a clear excess in the number of cases. Another point relat-
ed to the increase in the number of cases would be the
change in diagnostic criteria, accepting as microcephaly
cases of head circumference measuring less than 33 cm,
possibly explaining a situation of over-diagnosis. Another
relevant question, since the infection Zika virus in new-
borns and pregnant women were not confirmed by labo-
ratory tests at first, is that the history of nonspecific rash
referred to during pregnancy is subject to recall bias and
may have incurred potential misclassification regarding
exposure to Zika virus. Regardless of any controversies to
confirm, or not, the role of Zika virus in the genesis of cas-
es of microcephaly, measures to prevent infection with this
virus are necessary and unquestionable.