













 8 / 105
8 / 105

M
endes
and
L
usa
198
R
ev
A
ssoc
M
ed
B
ras
2016; 62(3):197-198
lar, and is limited laterally by the rectus abdominis mus-
cle and inferiorly by the inter-symphyseal band, where
the external urethral sphincter is inserted. The perineal
floor is compromised by the malformation, which ex-
plains the recurring rectal prolapse. The anus is more an-
terior compared to its original position in both sexes.
Boys present epispadias, short phallus, wide at its
base and with upward (dorsal) curvature. The urethra is
represented by exposed dorsal mucosa. Penis size is vari-
able, but is often small, imposing serious difficulties in
obtaining adequate phallus even after reconstruction.
The scrotum is split and the testicles are usually palpa-
ble (Figure 3). Cryptorchidism is rarely associated anom-
aly, and most commonly the testicles are located in the
external inguinal ring and can be descended into the tes-
ticular pouch. Inguinal hernia, probably related to the
fragility of the side of the abdomen, is common.
Typically, girls have bifid clitoris; the internal genita-
lia is normal, and vaginal and uterine abnormalities may
occur. The urethra is also epispadic and extremely short.
Differential diagnosis includes diseases that occur
with defect of the anterior abdominal wall, such as om-
phalocele, gastroschisis and cloacal exstrophy.
R
esumo
Extrofia vesical
A extrofia de bexiga é uma anomalia congênita rara decor-
rente de falha da fusão dos tecidos da linha média da pelve
durante a embriogênese e caracteriza-se por má-formação
da região inferior da parede abdominal, envolvendo o trato
geniturinário e o sistema musculoesquelético. Apresenta in-
cidência estimada de 1:30.000 a 1:50.000 nascidos vivos, sen-
do 2 a 3 vezes mais frequente no sexomasculino. A idade da
criança é importante e os melhores resultados são obtidos
quando o tratamento é realizado logo após o nascimento.
Palavra-chave:
extrofia vesical.
R
eferences
1. Beaty JH. Congenital and developmental anomalies of hip and pelvis In: Canale
TS. Campbell’s operative orthopaedics. 10.ed. St. Louis: Mosby, 2003. p.1118-9.
2.
Ramírez E, Calderón M. Osteotomía ilíaca en extrofia vesical. Rev Mex Ortop
Traumatol. 1997; 11(5):293-6.
3.
Segev E, Ezra E, Binyamini Y, Wientroub S, Ben-Chaim J. A combined vertical
and horizontal pelvic osteotomy approach for repair of bladder exstrophy:
the Dana experience. Isr Med Assoc J. 2004; 6(12):749-52.
4.
Frey P. Bilateral anterior pubic osteotomy in bladder exstrophy closure. J
Urol. 1996; 156(2 Pt 2):812-5.
5.
Satsuma S, Kobayashi D, Yoshiya S, Kurosaka M. Comparison of posterior
and anterior pelvic osteotomy for bladder exstrophy complex. J Pediatr
Orthop B. 2006; 15(2):141-6.
6.
Martín C, Darnell A, Durán C, Bermúdez P, Mellado F, Rigol S. Magnetic
resonance imaging of the intrauterine fetal genitourinary tract: normal
anatomy and pathology. Abdom Imaging. 2004; 29(3):286-302.
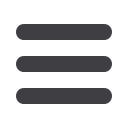
FIGURE 3
Coronal T2 MRI. Ectopic testes located in subcuta-
neous tissue, anterior surface of the thighs.