













 18 / 105
18 / 105

M
iranda
B
et
al
.
208
R
ev
A
ssoc
M
ed
B
ras
2016; 62(3):207-211
Oncology (Cacon). These recommendations are contin-
ually updated and integrated with other policies and
strategic actions for confronting chronic noncommuni-
cable diseases (CNCD)
7
and with home care services
(HCS).
8
Oncologic patients, especially those with advanced
disease, due to the natural history of their disease, anti-
cancer therapy and/or lack of control of symptoms, may
present complications or significant deterioration in their
clinical condition requiring emergency care. Therefore,
this action is a key part of a comprehensive care aiming
to improve quality of life and relief of suffering.
9
In relation to urgent and emergency services, cancer
patients face difficulties and challenges, although the pol-
icy states that the Cacon must operate 24 hours a day.
8
Urgent and emergency services should comply with
the health care model in force in Brazil, which today often
functions as access to health care. This is due to the low ef-
fectiveness of primary care and the difficulty of access to
high complexity services and hospitalization.
10
Neverthe-
less, the logic of emergency care escapes the basic princi-
ples of palliative treatment for patients at the end of life,
and can lead to increased and unnecessary suffering.
10,11
Considering the lack of local studies on this, our study
aims to analyze the clinical and sociodemographic pro-
file of cancer patients seen in the emergency service of a
Cacon, considering the availability of palliative care (PC)
and home care (HC).
M
ethod
This is a descriptive, cross-sectional study with an analyt-
ical component carried out at the emergency room (ER)
of the Instituto de Medicina Integral Prof. Fernando
Figueira (Imip), a teaching and research hospital that be-
longs to the oncology care network of the state of Per-
nambuco as a Cacon center.
The study population consisted of patients with can-
cer treated at oncological service and attended at ER for
oncologic monitored from September 2011 to December
2011, with length of stay >2 hours, aged 18 years or old-
er. The instrument used for data collection consisted of
a structured questionnaire with items on sociodemo-
graphic profile, and other specific questions on reason
for seeking emergency care, medical condition, diagno-
sis, staging, cancer treatment and monitoring in the PC
outpatient clinic and HCS. We conducted a pilot study
to test the instrument in early September 2011. After nec-
essary adjustments, data collection was held from Sep-
tember 20
th
to December 21
st
2011, every day (including
weekends and holidays), three times.
The database was built with double entry in the SQL
Server software and Frame Work application. Frequency
distribution tables, charts in Excel spreadsheet version 8.0,
and statistical tests (Student’s-t test for mean comparison
and chi-square test) were prepared using Epi Info 3.5.3.
This project was approved by the Ethics Committee
on Human Research of the Imip, no. 2426-11 and CAAE
no. 0085.0.099.000-11.
R
esults
191 medical reviews were performed including those of
20 patients who sought the ER service two times or more.
The maximum number of ER entries by a single patient
was 6, and 64.4% of the patients were female. Clinical and
sociodemographic variables are shown in Table 1.
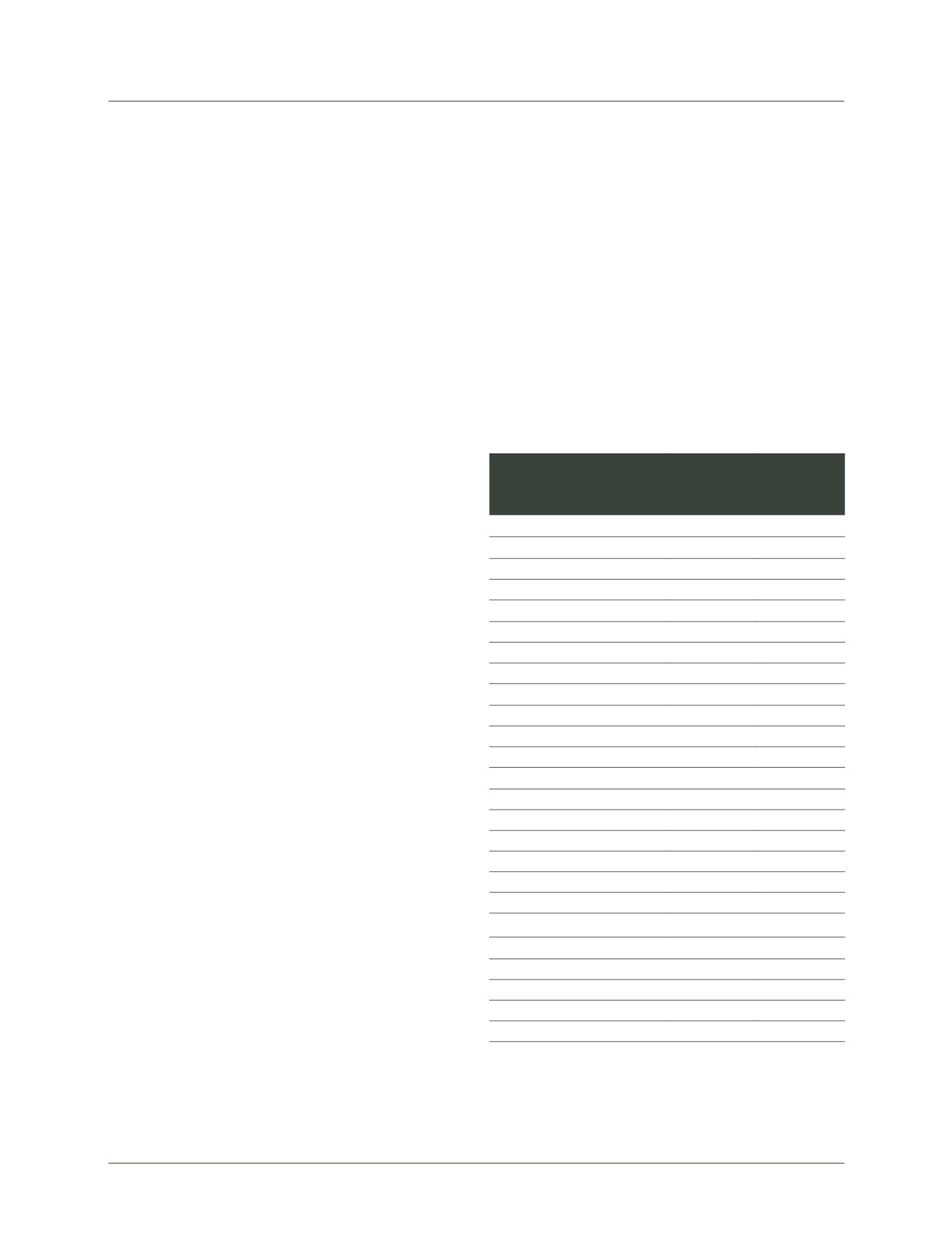
TABLE 1
Characteristics of cancer patients seen in the
emergency service of the Imip, and their progression. Recife,
2011.
Variables
n
%
Gender
Female
123
64.4
Male
68
35.6
Age (years)
≥ 60
91
47.1
40-59
69
35.7
18-39
30
17.2
Origin
Recife
71
37.2
GRA
73
38.2
Others
47
24.6
Type of treatment
None
78
39.5
Chemotherapy
60
30.3
Radiotherapy
19
9.6
Hormone replacement
16
8.1
Chemo and radiotherapy
11
5.5
Surgery
3
1.5
Others
11
5.5
Progression
Hospital discharge
86
45.0
Admission
97
50.8
Transfer
4
2.1
Death
4
2.1
GRA: great Recife area.
Most patients came from Recife and greater area (75.4%).
They were aged between 19 and 91 years, mean 57 years,
and 47.6% were older than 60. Among the identified clin-