














 95 / 100
95 / 100

M
icroscopic
colitis
: A
literature
review
R
ev
A
ssoc
M
ed
B
ras
2016; 62(9):895-900
897
may be absent in biopsies of the sigmoid colon or rectum,
emphasizing the importance of obtaining proximal colon
biopsies for the diagnosis of CC. In general, histopatho-
logical changes are restricted to the large intestine, al-
though thickening of the collagen layer may infrequent-
ly be found in the stomach, duodenum or terminal ileum.
13
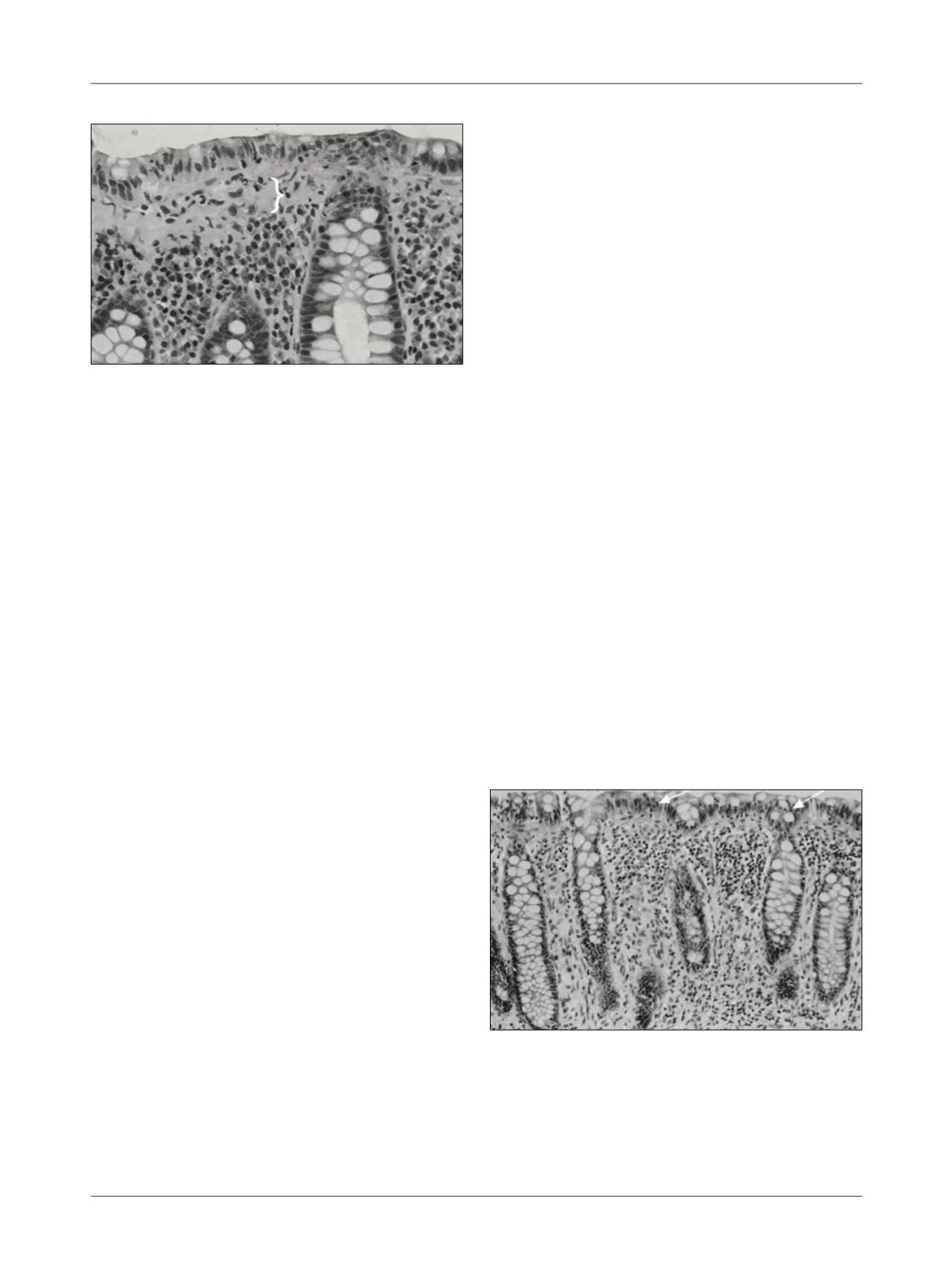
Meanwhile, in LC (Figure 2), we can observe an in-
crease in the number of intraepithelial lymphocytes (≥
20/100 surface epithelial cells), in conjunction with dam-
age to the surface of the epithelial cells and infiltration of
lymphocytes and plasma cells in the lamina propria. The
collagen layer, however, remains normal. In doubtful cas-
es, immunolabeling of CD3 T lymphocytes facilitates the
assessment of the amount of intraepithelial lymphocytes.
3,13
There are histological similarities between the two
forms of colitis, such as inflammation in the lamina pro-
pria essentially consisting of an increase in the number
of lymphocytes and plasma cells and epithelial damage.
4
T
reatment
The first step in treating patients with MC is to search for
exacerbating factors, such as dietary history in order to
search for foods that contribute to cause diarrhea, such
as dairy products in patients with lactose intolerance or
excessive consumption of dietetic products like caffeine
and alcohol.
1,2,13,14
It is also important to review the medication current-
ly used by the patient in order to search for drugs or sub-
stances that are causing or exacerbating the diarrhea in
MC.
1,5,8,14
Stopping smoking should be considered, al-
though the evidence for such is still weak.
5
Nevertheless,
most patients with MC require treatment.
1
Treatment of MC must take into account the severi-
ty of the symptoms, the impact on the patient’s quality
of life and the availability of data about the results of ran-
domized clinical trials. The main objective is to achieve
clinical remission and improve the patient’s quality of
life. It is not currently known whether histological remis-
sion is relevant to the recurrence rate. Therefore, it is un-
clear if this should be an important goal.
7
Antidiarrheal drugs such as loperamide are often used
in MC empirically in patients with mild diarrhea, but have
never been formally tested in randomized placebo con-
trolled trials. Clinical remission is rarely achieved and an
impact on colon inflammation is unlikely.
1,5,7
In 1998, Fine et al.
15
suggested the use of three bis-
muth subsalicylate tablets (262 mg/each), three times/
day in patients with mild symptoms or those that do not
respond to loperamide. However, in 2001, Pardi et al.
16
showed that most patients treated with this medication
showed a partial response.
Steroids are the most effective treatment in patients
with more intense symptoms and nonresponders to bis-
muth, with the use of budesonide as the best-document-
ed treatment.
1,9
Baert et al.,
17
Bonderup et al.
18
and Miehlke et al.
19
showed the efficacy of budesonide at a dose of 9 mg/day
for 6 to 8 weeks for the induction of clinical remission in
randomized placebo-controlled clinical trials on CC. Most
patients responded quickly to budesonide, and present-
ed a substantial improvement in quality of life and clin-
ical symptoms after 2 to 4 weeks of treatment. In a Co-
chrane meta-analysis conducted in 2009 by Chande et
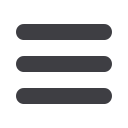
FIGURE 1
Collagenous colitis. In addition to the inflammatory
infiltrate, a thick band of subepithelial collagen can be observed
(brace).
Source: adapted from Pardi DS et al.
2
FIGURE 2
Lymphocytic colitis. Intraepithelial lymphocytosis
(arrows) can be observed, and mixed inflammatory infiltrate in the
lamina propria. With regard to the distinction between ulcerative
colitis and Crohn’s colitis, the architecture of the crypts is normal.
Source: adapted from Pardi DS et al.
2